Nervous System and Senses
2-D says, See me, down below, drinking sugar water.
I have chemoreceptors in my feet, so I can taste if I land on a flower
with nice, sweet nectar. Ms. Carter put my feet in the sugar water so I
could taste how sweet it was, and then I stuck my tongue in it and started
drinking. Yum!
Background Information:
Neuron with Schwann Cells around Axon
The nervous system consists of two types of cells. Nerve cells are called
neurons. Various support cells are associated with the neurons, most
typically, Schwann cells. The parts of a neuron include the
dendrite
which receives the impulse (from another nerve cell or from a sensory organ),
the cell body (numbers of which side-by-side form gray matter)
where the nucleus is found, and the axon which carries the
impulse away from the cell. Wrapped around the axon are the Schwann
cells, and the spaces/junctions between Schwann cells are called
nodes of Ranvier. Collectively, the Schwann cells make up the
myelin sheath (numbers of which side-by-side form white matter).

Cross-Section of Schwann Cell
Schwann cells wrap around the axon (like the camp food, pigs in a blanket).
Having an intact myelin sheath and nodes of Ranvier are critical to proper
travel of the nerve impulse. Diseases which destroy the myelin sheath
(demyelinating disorders) can cause paralysis or other problems. Schwann
cells are analogous to the insulation on electrical wires, and just as
electrical wires short out if theres a problem with the insulation, so also,
neurons cannot function properly without intact myelin sheaths.
The nervous system has three basic functions:
- sensory neurons receive
information from the sensory receptors,
- interneurons transfer and
interpret impulses, and
- motor neurons send appropriate
impulses/instructions to the muscles and glands.
A nerve impulse is an electrical charge that travels down the
cell membrane of a neurons dendrite and/or axon through the action of the
Na-K pump. Ordinarily, the inside of a neurons cell membrane is
negatively-charged while the outside is positively-charged. When sodium and
potassium ions change places, this reverses the inner and outer charges
causing the nerve impulse to travel down the membrane. A nerve impulse is
all-or-none: it either goes or not, and theres no halfway. However, a
neuron needs a threshold stimulus, the minimum level of stimulus
needed, to trigger the Na-K pump to go and the impulse to travel. A neuron
cannot immediately fire again; it needs time for the sodium and potassium to
return to their places and everything to return to normal. This time is
called the refractory period.
Click on this image to see the impulse travel down the axon.
A junction between two nerve cells or a nerve and a muscle
cell is called a
synapse.
In a synapse, various chemicals are used to transfer the impulse across the
gap to the next cell. These are collectively known as neurotransmitters,
and include such chemicals as dopamine (brain levels of which are low in Parkinsons
disease), serotonin, and acetylcholine (levels of which are low in
myasthenia gravis).
The Parts of the Nervous System
The nervous system can be subdivided several ways depending on
if one is looking at function or location:
| In terms of function, |
| ↙ ↘ |
Somatic NS
voluntary muscles and reflexes |
vs |
Autonomic NS
visceral/smooth and cardiac muscle
↙ ↘ |
| |
Sympathetic NS
increases energy expenditure
prepares for action
|
Parasympathetic NS
decreases energy expenditure
gains stored energy
|
| |
these have the opposite effects on the same organs
|
OR
| In terms of location, |
| ↙ ↘ |
Peripheral NS
sensory and motor neurons |
vs |
Central NS (CNS)
interneurons: brain and spine
covered with three membranes, the
meninges
inflammation of these is called
meningitis
brain has gray matter on outside and white in center
spine has white matter on outside and gray in center |
Most body organs/systems are enervated by both sympathetic
and parasympathetic nerves, and these have opposite effects on the various
organs. For example, the sympathetic NS prepares for action by increasing
heart and respiration rates. by telling the liver to release stored glycogen
as sugar, and by decreasing digestive processes. Conversely, the
parasympathetic NS stores energy by slowing heart and respiration rates, by
telling the liver to store up sugar as glycogen, and by increasing digestive
processes.
The Parts of the Brain:

Parts of the Brain
The brain consists of the
cerebrum
which is the large, anterior portion; the
cerebellum
which is the wrinkled-looking, posterior part; the
pons
which is the closest, larger bulge at the top of the spinal cord; and the
medulla
which is the farther, smaller bulge between the pons and the top of the
spinal cord; then the spinal cord starts after the medulla. Also
note under the cerebrum, the
optic chiasma,
the place where the optic nerves cross to the other side of the brain. The
cerebellum, medulla, and pons are collectively referred to as the
hindbrain. Many of their functions are involved in homeostasis,
coordination of movement, and maintenance/control of breathing and heart
rate. While a stroke in the cerebrum might result in partial paralysis, a
stroke in the hind brain is actually, potentially more dangerous becuase it
could knock out coordination of the cerebrums activities, or worse yet,
automatic control of breathing and/or heart beat. The midbrain is
responsible for receiving and integrating of information and sending/routing
that information to other appropriate parts of the brain. The forebrain
is composed of the cerebrum and related parts, and functions in pattern and
image formation, memory, learning, emotion, and motor control. In addition,
the right side functions more in artistic and spatial concepts, while the
left side controls speech, language, and calculations. Keep in mind that
motor skills are controlled by the opposite half of the brain, thus a
left-brain stroke would cause paralysis on the right side of the body.
Also, a left-brain stroke might cause problems with speech while a
right-brain stroke is more likely to cause abnormal/inappropriate emotional
responses.
Alzheimers, Prions, and Related Disorders
Scientists are increasingly discovering/suspecting that a
number of neurological diseases/disorders appear to be caused by something
called prions. Prions were only discovered in the 1980s. They are
molecules of protein that has become denatured/misfolded (has lost its normal,
native conformation), and thus, somehow, are self-replicating in that they
are able to trigger the matching, normal, correctly-folded proteins to
become misfolded, and those trigger more proteins to do the same, etc. Prions
are only protein, so are not alive. The first prion diseases discovered,
and thus, the most widely-studied are those that relate to a protein that
is nicknamed PrP (which is short for Prion Protein. The
normal form of this protein is called PrPC (where C stands for
Common or Cellular), while the infective, prion form is
called PrPSc because it was first fond in association with a
disease called Scrapie that occurs in sheep. PrPC is,
as mentioned, a normal protein which serves important functions in our
brains/neurons.
PrPSc causes a variety of neurodegenerative
(degeneration of the brain), and the incubation period appears to be from
5 to 20 years. However, in this case, incubation may be a bit of a
misnomer, because the PrPSc molecules arent just sitting around
waiting. Rather, undetected, theyre quietly causing more and more normal
PrPC molecules in the victims brain to turn into PrPSc,
causing increasing amounts of brain damage, until it gets to a point
where the loss of function becomes apparent. In sheep and goats, the
disease is called Scrapie, in cattle, its called Bovine Spongiform
Encephalopathy, also known as Mad Cow Disease. PrPSc also
causes similar brain diseases in mink, white-tailed deer and relative
species, cats, several other species of animals related to antelopes/cattle,
and ostriches. PrPSc also causes several forms of Spongiform
Encephalopathy in humans, including diseases known as Kuru and
Creutzfeldt-Jakob Disease (CJD).
PrPSc is communicable. One way it may be
spread/acquired is via consumption of dead animals that have PrPSc
in their bodies/brains. Kuru was found among certain peoples that are
native to the New Guinea highlands. The tradition of these people involved
eating the brains of their dead relatives to impart that persons wisdom
to his/her younger relatives, and unfortunately it was discovered that
practice transferred PrPSc to those people who ate infected
brain tissue, causing them, years later, to also develop and die from
Kuru. After researchers figured out what was going on, it was a delicate
situation to convince these people to abandon their long-standing, traditional
way of honoring their dead, but now that they no longer do so, they no
longer are plagued with Kuru. There is evidence that PrPSc may
also be spread via urine, saliva, and other body fluids from infected
animals, and there is some pretty-convincing evidence that it can also
be spread in manure of infected animals, which is a big concern since
feedlots full of cattle manure typically are located near water reservoirs
and manure was/is often used to fertilize crop fields. There is also
evidence that PrPSc may be spread via airborne, aerosol particles
(as in coughing, breathing, etc.). Preliminary research has shown that
prions may be transmitted through the use of hormones from PREgnant
MARe urINe given to human females to control their menstrual
cycles.
A number of years ago, in Great Britain, huge numbers of
cattle were put to death after the discovery of Mad Cow Disease in some
of them. The concerns were a) that the disease could spread from cow to cow
via manure, body fluids, etc., b) that since the diets of the cattle, who are
typically total vegans by nature, were being supplemented by cow chow
made from slaughter-house left-overs, the prions could be transferred that
way, and c) that humans who consumed meat from those cattle could possibly
become inoculated with PrPSc. A related, interesting topic
of discussion at that time was that of to pet food. Standards for what meat
goes into pet food production are less stringent that meat designated for
human consumption. Due to that, a couple of further concerns were raised.
Could pet cats and dogs be inoculated with PrPSc from eating
canned pet food (and could that be transferred to their people)?
Considering that numerous pet owners do taste the food they give to their
pets (pets dont need all the salt, garlic, etc., used to flavor their food
its there because the companies know people taste the food), and numerous
low-income people, perhaps especially the elderly, routinely eat canned pet
food because thats less expensive, more shelf-stable, and available in
smaller quantities than purchasing people-quality meats, could people
be inoculated with prions that way?
PrPSc is very resistant to normal sterilization
practices. It is resistant to inactivation by heat, formalin, or exposure
to UV light or x-rays. Prion-quality sterilization involves things like
immersion in sodium hydroxide (NaOH) in an autoclave (under heat and
pressure) for 30 to 60 min. Human-to-human transmission via organ
transplants and prion-contaminated brain electrodes has been observed. The
incidence of CJD among people who have previously had neurosurgery is higher
than among the general population.

Tau-Related Brain Degeneration
(anterior at top)
It has long been recognized that the amyloid-β plaques
found in Alzheimers Disease, the α-synuclein found in Parkinsons,
and phosphorylated tau (tau tangles) found in a number of neurological
disorders, including Alzheimers, Corticobasal Degeneration (CBD), etc., as
well as the superoxide dismutase 1 associated with amyotrophic lateral
sclerosis (ALS, Lou Gehrigs Disease) are
all misfolded forms of normal brain proteins. Tau, for example, is normally
a long, straight-stranded protein that helps microtubules in neurons to
do their jobs. When tau becomes phosphorylated, it crumples up into tangled
balls consisting of multiple strands of tau, and interferes with normal
microtubule structure and function. It has been known that tau tangles are
able to leave their neuron, travel to and into another neuron, and once
there, cause the tau in that neuron to also tangle, to the point that it
becomes possible to correlate the path of the spread of tau tangles in the
brain with the progression of Alzheimers symptoms. For a number of years,
in the 2000s, as these proteins were being studied, researchers initially
said this behavior was similar to the behavior of prions, but Im seeing
increasing numbers of recently-published (as of 2011, 2012, 2013, etc.)
articles that just out-and-out call all of these misfolded-proteins
prions. Researchers have injected purified tau and/or amyloid-β into
the bloodstream of mice, then several months later, found Alzheimers-type
changes in the mices brains, demonstrating that Alzheimers is communicable.
Thus, they have conjectured that blood
transfusions from someone with early-stage, undetected, asymptomatic
Alzheimers (or other degenerative neurological disease), surgical,
especially neurosurgical, equipment that has not been prion-sterilized,
and/or transplacental transfer from mother to baby in a pregnant woman
may, possibly serve as sources of prion inoculation in an
individual. Again, in their normal native conformation, these are all
important, useful brain proteins, but when they become denatured/misfolded,
they turn into infective prions.
So, what can be done to fight something that can only be
stopped by things like simultaneously soaking in lye and autoclaving? We
cant do that so someones brain! There is some research looking at the
possibility of using monoclonal antibodies that would tag tau
tangles, etc., for destruction by the persons immune system.
There is another treatment being tried by many people that
will not cure the neurological degeneration, but may help slow it down and
may help to keep neurons alive. As a bit of background, it turns out
that the insulin made by our pancreas does not cross the blood-brain barrier,
but rather, our brains make their own insulin. You may (hopefully) recall
that insulin is a hormone that helps/allows cells to take sugar (from the
bloodstream) into themselves so they can use it as a source of energy. It
turns out that, perhaps related in some yet-to-be-discovered way to the
presence/action of the tau tangles, neurons can be or can become
insulin-resistant, to the point where many researchers are now labeling
Alzheimers as Type III diabetes. The person does not have to also
have type I or type II diabetes, and may have a perfectly-normal blood-sugar
level. What insulin-resistance in neurons means is that the neurons dont
get the message and so cannot take sugar inside of themselves. Keep in
mind that, unlike Type I or Type II diabetes, it would do no good to treat
with supplemental insulin because it will not cross the blood-brain barrier.
Also, keep in mind that its not a blood-sugar issue, but rather, if the
neurons cannot take in sugar to use as fuel, they will, essentially, starve
to death. It has been observed that, in retrospect, many people who are
diagnosed with Alzheimers were, for years, super-sugar-junkies their
poor, starving neurons were sending out messages that they needed more
sugar, so eat lots more, but because the neurons were insulin-resistant,
none of all of that sugar ever got inside of them, so they just kept asking
for more.
Dr. Mary Newport,
a UC Med. School graduate, has pointed out that, back in caveman times, if
our bodies and especially our brains could use only sugar (glucose)
as a fuel, and given the insecurity, back then, of knowing when the next meal
would arrive, we wouldnt be here today. It turns out that our bodies and
brains (especially in tiny infants) can and do use other molecules, especially
including
medium-chain
triglycerides,
as fuel. According to information Dr. Newport has gathered and has personally
tested, she and many other people have found that feeding medium-chain
triglycerides (MCTs) (found in coconut oil, which is around 57 to 60% MCTs
and found at most grocery and health-food stores) to their loved ones who
have been diagnosed with Alzheimers (or other neurological diseases/disorders)
appears to feed the neurons and keep them alive (these oils do cross the
blood-brain barrier and do not require insulin to help them get into cells),
thereby slowing the
progression of the disease, and in some cases actually improving the
persons condition somewhat (see Dr. Newports pictures of her husbands
ability to draw a clock before and after initiating treatment with coconut
oil). If this topic is of interest to you, then Id
encourage you to check out her Web site (link above) and/or her book (link
on her Web site).
This, by the way, is a great example of how the Web has
changed the way medicine is (or should be or will be) practiced. In the past,
if a physician said that a patient had X disease, and the patient asked,
So, what can I do about it? and the doctor answered, Nothing, the patient
would have had to accept that and just dwindle away without a fight. Now,
when the doctor says, Nothing, people are getting online and doing their
own medical research to find out what other people out there are trying,
what seems to be working, and what doesnt, and then going back to tell their
doctor what they found out. In the case of using coconut oil, up until now,
there hasnt been a lot of official research done on that and not a lot
of data collected, and thus most doctors either havent heard about it, or
when told about it by patients, are highly skeptical, or may have heard so
many comments, stories, and testimonials to its value from patients that
theyre beginning to wonder. Finally, the researchers are catching up:
driven by the overwhelmingly-positive results reported by actual users, an
official research study on the efficacy of coconut oil/MCTs in treating
neurological disorders (Alzheimers) was just begun in Florida in 2012.
Coconut oil is a solid below 76° F, and a liquid above that
temperature. It can be used in place of butter or other oils in cooking.
Rather than putting butter on vegetables, pancakes, or oatmeal, people who
are trying to increase their MCT intake will use coconut oil. Coconut oil
can be used in place of salad oil or butter for grilling fish, frying
grilled-cheese sandwiches or pancakes, etc. Several companies make
a product thats like nut butter, only made out of coconut (one company,
Nutiva, calls theirs Coconut Manna other companies have different names
for it). A jar of that can be warmed slightly until gooey, mixed with a jar
of ones favorite nut butter, a package of unsweetened shredded coconut, and
any spices, etc., that are desired (cinnamon, cocoa nibs, etc., etc.),
poured into a knife-proof pan (glass or metal) and refrigerated. Once solid,
it can be cut up, and a chunk consumed whenever the nibbles strike.
Also (as per one of the charts in Dr. Newports book), goats milk, cheese,
and butter are higher in MCTs than cows milk, cheese, and butter.
A thought to consider: Recall, as mentioned above, that
someone may have prion-type molecules causing brain damage years before
so many neurons die that it becomes obvious, and it is discovered that they
have Alzheimers (or whatever) that has been eating away at their brain
for years. Because of that, Dr. Newport suggests that all of us may wish
to consider consuming coconut oil now.
Senses
We say we have five senses. Can you name them? Heres the
list of the five senses.
Sensory adaptation is a decrease in sensitivity during
continued stimulation. For example, can you hear the heating/cooling system
moving air? Are you aware of any rings you may be wearing?
Mechanoreceptors,
are stimulated by physical means such as touch, pressure, motion, or
stretching. Many of these are in the skin. Note that pressure-sensitivity
also includes sound receptors or ears, our sense of hearing, which is
actually a sensitivity to changes in air pressure.
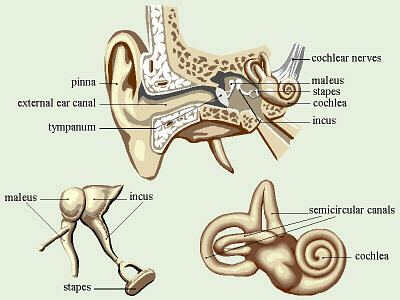
Structure of Ear
(clipart edited from Corel Presentations 8)
To hear a sound, the outer ear collects ripples or waves of compressed
air that we call sound, and passes them to the
tympanum.
Vibrations of the tympanum are transferred through three tiny bones in the
middle ear: the
malleus,
the
incus,
and the
stapes
to the inner ear, which contains a coiled organ called the
cochlea
where the actual receptors or nerve endings are located. These receptors are
fragile enough that exposure to very loud sounds can irreversibly damage them
(I have a friend who was a night-club musician for years and who has a lot of
hearing loss due to that),
and the more loud noises to which a person is exposed, the greater the
damage. People who frequently participate in rock music concerts have
noticeably reduced hearing ability. The inner ear also has a balance
sensor, which is composed of three loops at right angles to each other
called the semicircular canals.
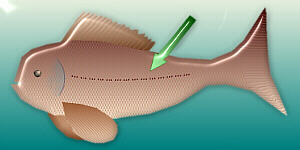
Lateral Line on Side of Fish
Fish hear via their lateral lines, a line of pressure sensors
running along each side of the fish that pick up pressure waves (= sound) in
water. When someone pounds on an aquarium, that creates waves of pressure
in the water that, to the fish, would be analogous to cupping your hands and
pounding on your ears NEVER POUND ON A FISH TANK! This, by the way, is the
same principle used when explosives are detonated in lakes to stun (or
kill) the fish so theyll float to the surface and can be more easily
collected for whatever purpose the human(s) involved had in mind (and
they probably were wearing ear/hearing protection).
Thermoreceptors
are temperature sensitive. Most of these are in our skin.
There are several kinds of pain receptors. Some are
sensitive to too much heat, others to too much pressure, etc. Sensitivity
of these (and other receptors) can be increased or reduced by certain drugs.
Painkillers are supposed to decrease the sensitivity of the pain receptors.
Our bodies natural endorphins function in this manner, and the
tendency to rub an injury stimulates the release of endorphins in that
location, lessening the pain. The stress of overexertion when doing
strenuous exercise also triggers the release of endorphins. Interestingly,
endorphins belong to the category of chemicals known as opiates, thus
are chemically related to opium, and also may potentially be addicting! It
is thought that a number of people who have to frequently do
strenuous exercise to feel good may actually be addicted to the endorphins
their bodies release under those circumstances they exercise to get high.
In general, it may not be a good idea to attempt to deaden any/all pain we
feel. Pain is a message from our bodies that something is wrong, thus can
be good at times when it reminds us to not do something we shouldnt. For
example, if a person with a back injury is on pain medication, the tendency
is for that person to overexert him/herself because it doesnt feel bad, and
perhaps injure the back further. If (s)he would not have been on painkillers,
(s)he would have gotten the message. Stop, its too much!

2-D Drinking Sugar Water with Her Feet in It
Chemoreceptors
include chemical senstivities like smell and taste. Interestingly, many
insects taste/smell with their feet and/or antennae. For example, if a
butterflys (or flys) feet are dipped in sugar water, it extends its tongue
(if its hungry). In humans, the senses of taste and smell are very complex.
There are both genetic and learned components to our sense of taste. One
famous demonstration frequently done in genetics classes is PTC
paper. This is a tissue paper impregnated with a chemical called
phenylthiocarbamide. About 70% of the people in the U.S. can taste this
substance, which has a horrible, bitter taste. About 30% of people who
taste this test paper, cannot taste the chemical and it just tastes like
paper. Preferences for certain tastes can also be acquired: people from
other countries are frequently repulsed by the amount of sugar in many foods
eaten here in the U.S. Perhaps tied in with that, it appears that tastes
change as a person matures. Strong tastes like mustard, onions, and radishes
are often repulsive to small children, yet many children who wont eat cooked
vegetables love the taste of raw vegetables fresh out of the garden. The
sense of taste is also influenced by the adequacy of ones diet, and people
who have a zinc deficiency tend to have taste buds that are considerably
less sensitive (a common complaint is I cant taste my food). Smoking
also tends to obliterate the unique tastes of foods, and people who quit are
often amazed at how different, how much better their food tastes. Similarly,
people who unthinkly add salt to everything are so used to everything tasting
like salt that when they have to or choose to reduce their salt consumption,
they frequently are amazed at how different all their foods taste.
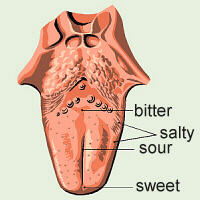
Tongue
(clipart edited from Corel
Presentations 8)
Different areas of the human tongue have sensitivities to different tastes.
Each of these areas contains proportionately more of certain chemoreceptors.
Typically, the middle-front of the tongue is more sensitive to sweet tastes,
the sides to salty tastes, the center-back to sour tastes, and the very back
to bitter tastes. One old herbal remedy for sore throat is tea made from
licorice root. I have noticed, when I drink this tea, when it comes into
contact with most of the taste sensors on my tongue, it just tastes like
water, but as I swallow it, it has a fairly strong, sweet taste very far
back on my tongue, down in my throat, where nothing else Ive ever eaten
triggers a response. I have never seen any discussion of this in the
literature.
Electromagnetic
receptors include sensitivities to light, including light we humans
cannot see, as well as things like electric and magnetic fields. Many
animals can see colors of light we cant (infrared, ultraviolet). Some
animals, like whales, can sense gravity, variations in the Earths
magnetic field, and use that in navigation.
Our eyes need vitamin A as the precursor to our visual
pigment. This pigment absorbs light energy and changes it to chemical
energy, then transfers an electrical impulse to the appropriate nerve
endings. This pigment is destroyed in the process and must be regenerated.
When a person spends time in the dark, part of the acclimation process is
synthesizing more visual pigment to increase the eyes sensitivity.
Therefore, if you get up in the middle of the night for a snack, you can
probably see better if you dont turn on more than just a night light to
navigate safely. If you turn on a lot of bright lights, much of the visual
pigment accumulated in your eyes will be destroyed, and when you turn out
the lights to go back to bed, you wont be able to see in the dark.
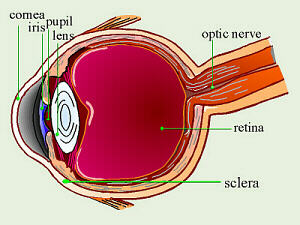
Eye
(clipart edited from Corel Presentations 8)
The parts of the human eye include the
cornea
covering the front, the
pupil
which is the opening in the center of the eye, the size of which is
controlled by the
iris,
and the
lens,
which focuses light onto the
retina,
which contains the
photoreceptors.
The white of the eye is the
sclera.
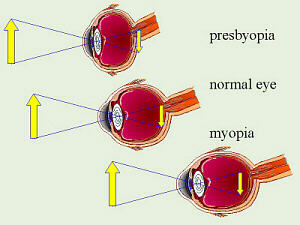
Near- and Farsightedness
(clipart edited from Corel Presentations 8)
The eyes of a person who is nearsighted (has
myopia)
are out of round such that they are too long front-to-back, thus an image is
in focus somewhere in the middle of the fluid in the eye. The eyes of a
person who is farsighted (has
presbyopia)
are out of round such that they are too short front-to-back, and the image
is in focus somewhere behind the eyeball. Note that the lens flips the
image over upside down, and as our brains process the information, the
image is flipped back, right-side up. Experiments were done in which people
were asked to wear special glasses that made everything look upside down, and
after a time, their brains learned to compensate and things, once again,
looked right-side up.

Sally Looking Forward

Sally Looking Sideways
An animal that is potential prey for another animal has its
eyes on the sides of its head and the eyes operate independently, giving the
animal nearly 360° vision to better watch for danger. A
predator
has its eyes on the front of its face, giving it excellent
binocular
vision for depth perception and judging distance to prey. An interesting
combination of these traits can be found in a chameleon (not an anole).
Chameleons eat insects, so need binocular vision to capture dinner, but are
also potentially dinner for someone else. They have their eyes on the sides
of their heads, but the eyes stick out and can swivel around. Chameleons can
use their eyes independently to watch for predators, yet when a potential
meal hops into sight, can focus both eyes on the insect to judge the
distance before flicking out a sticky tongue to catch it. Interestingly,
because of the location and mobility of a chameleons eyes, it can
rotate its eyes backwards, and have binocular vision behind its head!
Chickens, also, have their eyes on the sides of their heads, and they work
independently to watch for predators, but chickens use their binocular
vision to focus on the food theyre about to pick up.
Another light-sensitive organ that we are only beginning to
understand is the pineal gland. This organ manufactures melatonin in
response to darkness, thus the shorter the day (like in winter) the more
melatonin is secreted. In many animals, the pineal gland is located just
under the skin somewhere on the head, and is directly stimulated by light.
Some lizards even have a third eye! In humans, the pineal gland is inside
the skull and it is thought that it receives it stimuli from nerves from the
eyes. Some people make too much melatonin in the winter, making them sleepy
and/or depressed. This is called seasonal affective disorder (SAD)
and is treated by having the person spend a certain number of hours each day
in front of bright lights. There is also a drop in melatonin production at
puberty, and it is thought that these may be related. Studies have been done
on blind girls (with a form of blindness in which no impulses can travel down
the optic nerve and reach the brain and pineal gland), which showed that
these girls tended to have higher levels of melatonin for a longer time,
resulting in a delay in the onset of puberty. While some older people, who
dont make very much melatonin, thus dont sleep well, might benefit from a
melatonin supplement, Im leery of the recent melatonin craze in this country.
When so many people apparently are suffering from SAD, I question the wisdom
of purposly ingesting more melatonin.
References:
Berkow, Robert, ed. 1987. The Merck Manual. 15th Ed. Merck, Sharp & Dohme, Rahway, NJ.
Berkow, Robert, ed. 1999. The Merck Manual. 17th Ed. Merck, Sharp & Dohme, Rahway, NJ.
Borror, Donald J. 1960. Dictionary of Root Words and Combining Forms. Mayfield Publ. Co.
Campbell, Neil A., Lawrence G. Mitchell, Jane B. Reece. 1999. Biology, 5th Ed. Benjamin/Cummings Publ. Co., Inc. Menlo Park, CA. (plus earlier editions)
Campbell, Neil A., Lawrence G. Mitchell, Jane B. Reece. 1999. Biology: Concepts and Connections, 3rd Ed. Benjamin/Cummings Publ. Co., Inc. Menlo Park, CA. (plus earlier editions)
Marchuk, William N. 1992. A Life Science Lexicon. Wm. C. Brown Publishers, Dubuque, IA.
Newport, Mary T.
2013. Alzheimers Disease: What If There Was a Cure?, 2nd Ed. Basic Health Publ, Inc. Laguan Beach, CA.
Prusiner, Stanley B. 2014. Madness and Memory. Yale Univ. Press. New Haven, CT.
plus a number of Web-based references, including:
http://en.wikipedia.org/wiki/prion more info on prions
http://en.wikipedia.org/wiki/Corticobasal_degeneration is about corticobasal degeneration
http://www.ncbi.nlm.nih.gov/sites/entrez?db=pubmed&uid=16817199&cmd=showdetailview is about iron sequestration
http://en.wikipedia.org/wiki/Tauopathy is about tauopathy
http://www.ncbi.nlm.nih.gov/pubmed/10967355 is about tauopathy
http://en.wikipedia.org/wiki/Tau_protein is about tau protein
http://scienceindex.com/stories/1539256/Hyperphosphorylated_paratarg7_a_new_molecularly_defined_risk_factor_for_monoclonal_gammopathy_of_undetermined_significance_of_the_IgM_type_and_Waldenstrom_macroglobulinemia.html another hyperphosphorylated protein may be involved in MGUS
http://scienceindex.com/stories/2062855/Herpes_simplex_virus_type_1_induces_nuclear_accumulation_of_hyperphosphorylated_tau_in_neuronal_cells.html Herpes simplex type 1 may trigger production of phosphorylated tau
http://www.smartplanet.com/blog/savvy-scientist/infectious-proteins-on-the-brain-alzheimers-and-prions/346 tau tangles act like/are prions
http://news.bbc.co.uk/2/hi/health/8084787.stm tau can spread through the brain
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3015202/ info on tau, amyloid-β and prions
http://www.ncbi.nlm.nih.gov/pubmed/20021333 more on tau, amyloid-β, and prions
http://www.ncbi.nlm.nih.gov/pubmed/22365536 in vivo spreading of tau pathology
http://cen.acs.org/articles/90/i27/Alzheimers-Prion-Connection.html potential for tau prions to be spread via transfusion
http://web.ebscohost.com/abstract?direct=rue&profile=ehost&scope=site&authtype=crawler&jrnl=19326203&AN=55701005&h=i8tNB8eTAwM75C2MksknnTNKb7xVlHQ3RJXiv17dYJCrg3nOvWsja4%2bkVmB7Bk3rDIKwbEeajZDdKIO2ashNnA%3d%3d&crl=c amyloid-β is communicable
http://www.alzforum.org/new/detail.asp?id=2792 anti-tau monoclonal antibodies
http://www.faqs.org/patents/app/20120087861 anti-tau antibodies
http://askgeorgie.com/?p=5231 neurons can use lactate
http://www.jneurosci.org/content/31/13/4768.full.pdf neurons can use lactate
http://www.jneurosci.org/content/30/42/13983.full.pdf neurons can use lactate
http://www.news-medical.net/news/20120502/Grape-derived-compound-may-prevent-neurodegenerative-disorders-involving-tau-neuropathology.aspx is about use of a grape-derived extract that may be beneficial
http://www.jimmunol.org/content/183/9/5917.full.pdf use of cinnamon vs. amyloid-β prions
http://www.google.com/patents/EP2349301A2?cl=en use of cinnamon to treat amyloid-β prions
http://www.life-enhancement.com/magazine/article/2531-the-anti-alzheimers-power-of-whole-turmeric turmeric is anti-inflammatory, and therefore may be of use

Copyright © 1996 by J. Stein Carter. All rights reserved.
This page has been accessed  times since 14 Mar 2001.
times since 14 Mar 2001.